


Department of Dermatology and Allergology, Helsinki University Hospital, Meilahdentie 2, FIN-00250 Helsinki, Finland. *E-mail: alexander.salava@hus.fi
Accepted Dec 22, 2020; Epub ahead of print Dec 29, 2020
Acta Derm Venereol 2021; 101: adv00368
doi: 10.2340/00015555-3739
There is substantial need for effective treatments in pediatric AD (1). Mild topical corticosteroids and basic emollients are used as first-line. In non-responsive cases and frequent relapses, topical calcineurin inhibitors are recommended (2). For children over 2 years of age 0,03% tacrolimus ointment and 1% pimecrolimus cream have been approved (3). 0,1% tacrolimus ointment has been used off-label in pediatric AD (4), but there is still limited data regarding long-term treatment in children under 2 years of age (5). We analysed the use and safety data of topical tacrolimus in small children with AD and compared the usage with topical corticosteroids.
Interim analysis of a three-year follow-up study (4) was conducted, comparing 2 treatment modalities; tacrolimus ointment (both 0.03% and 0.1%) and topical corticosteroids (mild and mid-potency), in a cohort of 1 to 3 year old children. This was a randomized non-blinded follow up study with a one week wash-out period.
A total of 152 children with moderate to severe AD (Rajka and Langeland Eczema Severity Score) (4) were randomized for topical corticosteroids (hydrocortisone 1% and if needed hydrocortisone-17-butyrate cream) or topical tacrolimus (0.03% and if needed 0.1% ointment). There was a drop out of 15 patients during the first year due to nonadherence. Patients were advised to use topical corticosteroids twice per day for courses of 3-5 days or topical tacrolimus twice daily until the skin has cleared and thereafter twice per week if needed. Clinical assessment (including use of topical treatment) and assessment of severity were performed after the first week, at months 1, 3, 6, 9 and 12 and thereafter every 6 months.
At baseline, blood eosinophil count, total serum IgE, specific IgE antibodies (aeroallergens and food allergens) and skin prick tests were measured to investigate if early signs of atopy predict response to treatments. The cohort is characterized in detail in a former publication (4).
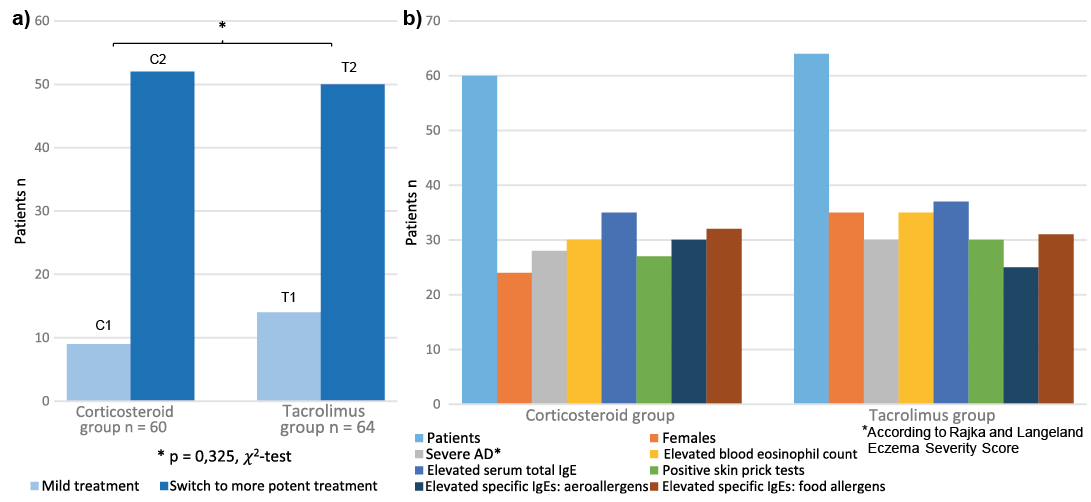
Fifty-one patients (85.0%) in the corticosteroid group (n = 60) and 50 (78.1%) in the tacrolimus group (n = 64) needed to switch to a more potent treatment. There were no significant differences between groups (p = 0.325, χ2-test; Fig. 1).
Fig. 1. Comparison of treatment groups. (a) Switch to more potent treatment. (b) Group characteristics at baseline; T1=0.03% tacrolimus ointment only; T2=0.03% and 0.1% tacrolimus ointment; C1: hydrocortisone 1% cream only; C2: hydrocortisone and hydrocortisone-17-butyrate-cream.
Disease severity and high Eczema Area and Severity Index (EASI) score predicted the need for more potent treatment (p = 0.009, Mann–Whitney U test). Switch to more potent treatment was due to poor treatment response in localized body sites (limbs, trunk, lichenified areas) or to frequent relapses. The switch to a more potent treatment was mostly needed on the extremities. If the patients needed a more potent treatment they usually needed it during the first follow-up year. Here, the treatment was switched to either hydrocortisone-17-butyrate cream (corticosteroid group) or tacrolimus 0,1% ointment (tacrolimus group). Characteristics of the treatment groups are shown in Table SI. Comparisons of the treatment groups are shown in Table SII and Fig. 2.
Fig. 2. Comparison of group characteristics at baseline. (a) Eczema Area and Severity Index (EASI) score. (b) Blood eosinophil count (aReference values for blood eosinophil count: 1 month – 1 year: 0.2–1.7 E9/l; 2–4 years: 0–0.30 E9/l). (c) Total serum IgE (bReference values for total serum IgE: 6 months–1 year 0–70 kU/l; 2–3 years 0–110 kU/l; 4–7 years 0–130 kU/l). (d) Signs of early IgE-mediated sensitization (cElevated serum total IgE and/or elevated specific IgEs to aeroallergens or food allergens and/or positive skin-prick tests); mild treatment: hydrocortisone 1% cream or tacrolimus 0.03% ointment only; Switch to more potent treatment: 0.03% and 0.1% tacrolimus ointment or hydrocortisone and hydrocortisone-17-butyrate-cream.
In our experience many small infants and toddlers with moderate to severe AD need an off-label use of more potent topical tacrolimus (0.1% ointment) or corticosteroid treatment (mid potency corticosteroids) to control the disease (6). Milder treatment may often not be sufficient with a risk of disease chronicity (7, 8).
Pediatric patients with moderate or severe AD may be undertreated due to fear of adverse effects (9, 10). Both hydrocortisone 1% cream and 0.03% tacrolimus ointment were in our cohort insufficient to control more severe AD. In addition, prior to study inclusion, many of the patients were insufficiently treated, often mostly with emollients.
Compliance issues and parental collaboration are recognized challenges in pediatric AD, which affects the quality of life of patients and their families (11, 12). In severe AD, the incidence of lymphoma might be increased in later life (13).
There have been concerns associated with the use of topical tacrolimus and corticosteroids in infants (14). However, intermittent topical mid-potency corticosteroids do not pose a high risk for adverse effects small infants and toddlers (15). Based on the official approval and treatment guidelines 0.1% tacrolimus ointment is not recommended for patients under the age 15 years (2).
In our patient cohort, long-term treatment with tacrolimus 0.1% ointment was safe and effective in pediatric AD (4). Systemic exposure to tacrolimus was not significant. The topical treatment was well tolerated, with side effects like pruritus and burning sensation mostly disappearing after continuous use. Many patients required a switch to a more potent topical treatment, mostly during the first year of follow up. We encourage this in cases of poor response to first line treatments, frequent disease flares and lichenified lesions on the extremities (7, 14).
In conclusion, our cohort of small infants and toddlers with moderate and severe AD seemed to be undertreated and there was a substantial need the switch to a more potent treatment (4, 6). Our observations do not provide direct evidence that pediatric atopic dermatitis is undertreated and more studies are needed to confirm our observations representing the situation in Finland. There might also be an increased risk of disease chronicity and other co-morbidities (11, 12). Our study shows that small infants with treatment refractory atopic dermatitis profit from the switch to a more potent topical treatment, i.e. mid-potency corticosteroids or 0.1% tacrolimus.
The authors would like to thank Anssi Koivuselkä for assistance.
Patient and parental advice, dermatological treatments and follow-up visits were carried out at the Skin and Allergy Hospital, Helsinki University Hospital, Finland. The study was approved by the Ethics Committee of Medicine of the Hospital District of Helsinki and Uusimaa (HUS), Finland. The patients and parents in this manuscript provided written informed consent to publication of their case details.
The work was supported by The Pediatric Research Foundation, Helsinki University Central Hospital Research Fund, Sigrid Juselius Foundation, Päivikki and Sakari Sohlberg Foundation, Finnish Dermatological Society, Allergy Research Foundation, Väinö and Laina Kivi Foundation, Orion Research Foundation, Ida Montin Foundation, Orion Pharma Finland and Astellas Pharma. The sponsors had no influence on the study.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize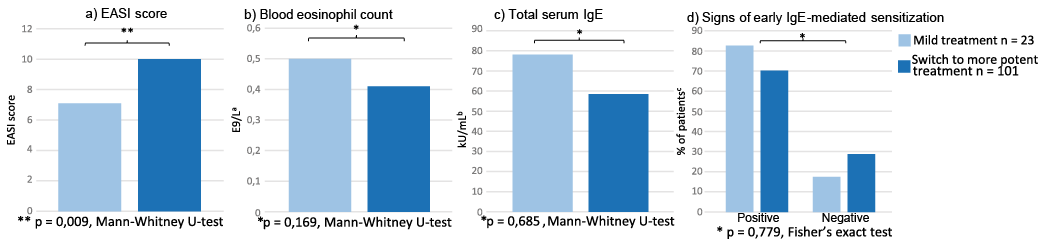 Click to show fullsize
Click to show fullsize